Medicaid billing is not like commercial insurance billing. It’s not even like Medicare billing. It has its own structure, its own rules, and its own frustrations.
If you treat Medicaid patients, you already know this. Payments are lower. Documentation standards are strict. Each state runs its program differently.
And small mistakes can delay reimbursement for weeks.
But here’s the truth. Medicaid can still be financially viable if you bill it correctly, document thoroughly, and understand how your state program works.
This guide walks you through Medicaid billing from enrollment to reimbursement, with real-world clarity. No fluff. Just what providers and billing teams need to know.
What is Medicaid?
Medicaid is a joint federal-state program that provides health coverage to low-income individuals, children, pregnant women, seniors, and people with disabilities.
While the federal government sets broad rules through the Centers for Medicare & Medicaid Services (CMS), each state administers its own Medicaid program.
That means Medicaid billing rules in Texas are not identical to those in Florida or California.
Fee schedules vary. Prior authorization rules differ.
Some states use heavily managed care models. Others rely more on fee-for-service structures.
If you bill Medicaid, your first responsibility is understanding your state’s program.
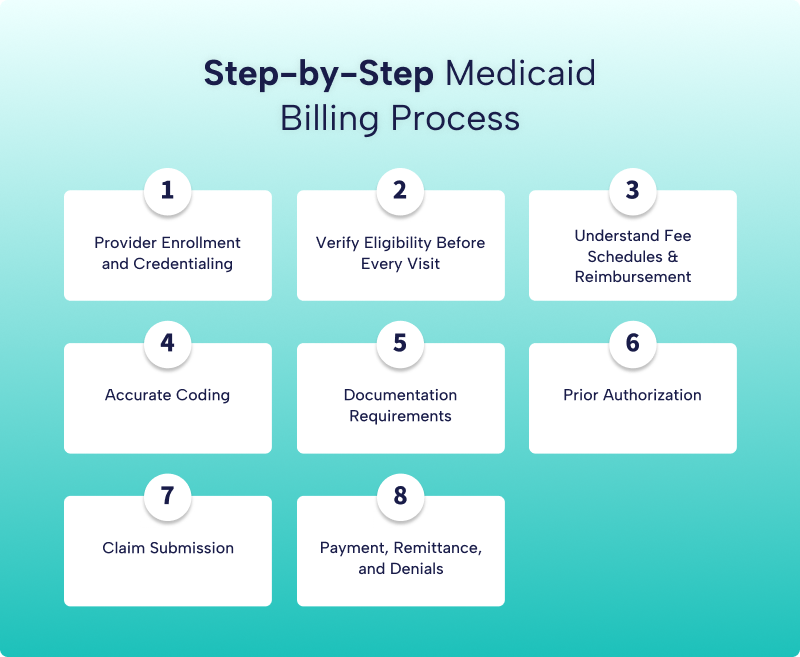
Step-by-Step Medicaid Billing Process
Many practices focus heavily on coding, but the billing process actually starts much earlier. It begins with patient scheduling and eligibility verification. It moves through documentation, coding accuracy, claim submission, and finally payment reconciliation. Every phase connects to the next.
- If your front desk skips eligibility verification, billing suffers.
- If documentation lacks medical necessity, coding suffers.
- If coding is inaccurate, reimbursement suffers.
That’s why understanding the full workflow matters. When your team sees Medicaid billing as a coordinated system rather than isolated tasks, denial rates drop, and cash flow stabilizes.
Now, let’s walk through the Medicaid billing process, so you can see exactly where risk lives and where revenue is protected.
Step 1: Provider Enrollment and Credentialing
Before you submit a single claim, you must be properly enrolled in Medicaid in your state. This process includes:
- Completing state Medicaid enrollment
- Obtaining a National Provider Identifier
- Registering taxonomy codes correctly
- Linking your group and individual NPIs
- Enrolling in Medicaid managed care plans if required
Here’s where many practices make mistakes.
They enroll in fee-for-service Medicaid but forget to credential with the state’s managed care organizations.
They claim, then deny, because that specific plan does not recognize the provider.
If your state uses managed care, you must contract with each Medicaid MCO separately.
Step 2: Verify Eligibility Before Every Visit
Medicaid eligibility changes frequently. A patient covered last month may not be covered today.
Always verify eligibility before the visit. Not once a year. Every single time.
Check:
- Active coverage status
- Managed care plan assignment
- Copay requirements
- Service limits
- Referral requirements
If you skip this step, you risk providing care that won’t be reimbursed.
Step 3: Understand Fee Schedules and Reimbursement
Medicaid reimbursement rates are generally lower than those of Medicare or commercial payers. Many states base rates loosely on Medicare’s physician fee schedule but apply percentage reductions.
For example, if Medicare pays $100 for a service, your state Medicaid may reimburse $60 to $80, depending on the state.
Before accepting large Medicaid volumes, review:
- Your state Medicaid fee schedule
- Global surgical packages
- Bundled services
- Evaluation and management rate
- Procedure reimbursement differences
Knowing your actual reimbursement helps you make staffing and scheduling decisions.
Step 4: Accurate Coding
Medicaid requires proper coding using:
- ICD 10 diagnosis codes
- CPT procedure codes
- HCPCS codes when applicable
- Modifiers when required
Common Medicaid billing issues include:
- Missing modifiers
- Incorrect place of service codes
- Unbundling services
- Billing non-covered services
- Using outdated codes
Many states enforce strict bundling edits. For example, certain minor procedures may be bundled into evaluation and management visits unless documentation clearly supports separate billing.
Always review your state Medicaid provider manual for coding specifics.
Step 5: Documentation Requirements
Documentation must fully support medical necessity. Medicaid programs are aggressive in denying services that do not meet medical necessity criteria.
Your documentation should clearly include:
- Chief complaint
- History and exam findings
- Assessment and diagnosis
- Plan of care
- Time when relevant
- Procedure details when applicable
For procedures, document:
- Indications
- Technique
- Anesthesia if used
- Complications
- Post-procedure instructions
If it isn’t documented, it didn’t happen. Medicaid audits follow that rule strictly.
Step 6: Prior Authorization
Many Medicaid services require prior authorization. This is especially common for:
- Imaging
- Physical therapy
- Durable medical equipment
- Surgical procedures
- Behavioral health services
Submitting claims without prior authorization when required will almost always result in denial.
Build internal workflows so your staff checks authorization requirements before scheduling certain services.
Step 7: Claim Submission
Claims are submitted electronically through clearinghouses or directly to the state Medicaid portal or managed care organization.
Key claim elements include:
- Correct Medicaid ID number
- Accurate NPI and taxonomy
- Proper place of service
- Correct diagnosis pointers
- National drug codes, when required
- Authorization numbers, if applicable
Small errors, such as missing taxonomy codes or incorrect rendering provider data, frequently trigger denials.
Medicaid Claim Submission Systems and Clearinghouses
Medicaid claims are typically submitted electronically through clearinghouses or directly through state Medicaid portals and managed care organization systems.
Clearinghouses act as intermediaries that:
- Validate claim data before submission
- Apply payer-specific edits
- Reduce rejections through claim scrubbing
- Provide real-time feedback on errors
Many practices rely on clearinghouse integrations with their practice management systems to streamline submissions and improve clean claim rates.
However, Medicaid managed care plans may require direct portal submissions for certain claim types, authorizations, or corrected claims.
Understanding where and how to submit each claim is essential. Submitting to the wrong channel can delay processing or result in automatic rejection.
Step 8: Payment, Remittance, and Denials
Once processed, Medicaid sends an electronic remittance advice. Review this carefully.
Common denial reasons include:
- Eligibility not active
- Authorization missing
- Non-covered service
- Coding mismatch
- Duplicate claim
- Exceeded service limits
Denial management is not optional. Practices that ignore denials lose revenue.
Build a process to:
- Review denials weekly
- Correct and resubmit quickly
- Appeal when appropriate
- Track denial patterns
If the same denial appears repeatedly, it’s a workflow issue.
How Medicaid Billing Impacts Your Practice Revenue
Medicaid billing is not just an administrative process. It directly affects your practice’s cash flow, staffing efficiency, and long-term sustainability.
Because Medicaid reimbursement rates are lower, even small inefficiencies can have a significant financial impact. Delayed claims, repeated denials, or incorrect coding can reduce already tight margins.
For example:
- A denied claim delays revenue by weeks or months
- Reworking claims increases administrative costs
- Underbilling reduces revenue on every visit
Practices that implement structured workflows, accurate coding, and proactive denial management consistently see:
- Faster reimbursement cycles
- Higher clean claim rates
- Improved revenue predictability
Medicaid becomes financially sustainable only when billing is handled with precision.
Medicaid Managed Care vs. Fee-for-Service: Key Differences
If you bill Medicaid, you need to know which model you’re dealing with. This is not a small detail. It changes how you submit claims, how you get paid, and how you handle denials.
Most states originally operated under a traditional fee-for-service structure. In that model, the state Medicaid agency pays providers directly for each covered service. You submit a claim. The state processes it. You get paid based on the state’s published fee schedule.
Over time, many states shifted to Medicaid managed care. Under this structure, the state contracts with private insurance companies to manage benefits for Medicaid members. These companies are called managed care organizations (MCOs).
In a fee-for-service, you deal with one payer, the state Medicaid agency. In managed care, you may deal with three, five, sometimes even ten different MCOs in the same state.
That changes everything.
Different fee schedules
Each Medicaid MCO may pay different rates for the same CPT code. One plan might reimburse 85 dollars for a level 3 office visit. Another might pay 72. If your contract is not loaded correctly into your system, you won’t catch underpayments.
Always load each MCO’s fee schedule separately. Do not assume parity across plans.
Different prior authorization portals
In a fee-for-service model, you usually submit prior authorizations through the state’s Medicaid portal. In managed care, every MCO has its own authorization system. Some use proprietary portals. Others use third-party vendors.
If your staff submits an authorization to the wrong portal, the service may be automatically denied. And most plans will not excuse that mistake.
Different timely filing limits
Timely filing limits vary. Fee-for-service Medicaid might allow 180 days from the date of service. An MCO could allow 90 days. Another might allow 120.
Miss that window, and you lose the claim. No exceptions in most cases.
Track timely filing limits per payer inside your practice management system. Do not rely on memory.
Different appeal processes
Appeals in fee-for-service usually follow a standardized state process. Managed care plans set their own appeal timelines, forms, and documentation requirements.
One plan may require appeals within 30 days. Another may allow 60. Some require paper submission. Others require portal uploads.
You must treat each Medicaid MCO like a separate commercial payer with its own policies, workflows, and contract terms. If you treat them as “just Medicaid,” you’ll see preventable denials stack up fast.
Common Medicaid Billing Mistakes That Lead to Denials
Even experienced practices make avoidable mistakes when billing Medicaid. These errors often lead to delays, denials, and lost revenue.
The most common issues include:
Incorrect Managed Care Plan Billing
Submitting claims to the wrong Medicaid MCO results in automatic denials.
Missing Prior Authorization
Many services require prior authorization. Claims without it are rarely paid.
Eligibility Not Verified
Medicaid coverage can change monthly. Failure to verify eligibility leads to denied claims.
Coding and Modifier Errors
Incorrect CPT, ICD-10, or modifier usage can trigger payer edits.
Missing or Incorrect Provider Information
Errors in NPI, taxonomy, or rendering provider details often result in claim rejection.
Medicaid Billing Challenges and Solutions
Medicaid billing looks simple on the surface. Lower reimbursement, state program, standardized rules. That assumption causes problems fast.
In reality, Medicaid is one of the most complex payers to administer. Rules change often. Managed care adds layers. Audit exposure is real.
Below are the most common challenges medical practices face, along with realistic solutions you can implement.
Low Reimbursement Rates
Medicaid typically reimburses less than commercial insurance and sometimes less than Medicare. For example, an office visit that costs 120 dollars under a commercial plan might cost 70 to 85 dollars under Medicaid, depending on the state.
When your payer mix is high in Medicaid patients, margins get tight. Practices feel pressure quickly.
The Solution
- Optimize coding accuracy. Underbilling hurts even more when rates are already low. Ensure documentation supports appropriate E and M levels.
- Track underpayments. Many practices assume Medicaid always pays correctly. That is not always true. Load fee schedules accurately into your system and reconcile payments monthly.
- Improve operational efficiency. Shorten claim submission cycles. Reduce rework. The faster clean claims go out, the faster revenue comes in.
- Monitor payer mix. If Medicaid volume exceeds sustainable thresholds, adjust scheduling templates or expand service lines with better reimbursement.
Complex Managed Care Variations
Medicaid Managed Care Organizations operate like separate insurance companies. Each has:
- Different fee schedules
- Different prior authorization requirements
- Different claim edits
- Different appeal deadlines
Staff confusion leads to denials. Denials lead to delayed cash flow.
The Solution
- Create a centralized Medicaid payer matrix. This document should list:
- Each MCO
- Timely filing limits
- Authorization portals
- Contact numbers
- Appeal timeframes
- Key billing rules
- Update it quarterly.
- Train staff to verify plan details at every patient visit. Do not rely on assumptions. Eligibility and plan assignments change often in Medicaid populations.
- Treat each MCO like a unique commercial payer. Build workflows accordingly.
Frequent Eligibility Changes
Medicaid eligibility can change monthly. Patients may lose coverage, switch MCOs, or move into different benefit categories.
If you do not verify eligibility at each visit, claims will be denied for inactive coverage.
The Solution
- Verify eligibility 48 hours before appointments and again on the day of service.
- Automate eligibility checks through clearinghouse integrations when possible.
- If eligibility changes mid-treatment cycle, adjust billing immediately. Do not continue submitting claims to the previous plan.
Prior Authorization Delays
Many Medicaid services require prior authorization, especially imaging, therapies, specialty visits, and durable medical equipment.
Submitting incomplete or incorrect authorizations leads to denials that are difficult to overturn.
The Solution
- Assign clear ownership of authorizations. One team or a designated individual should manage tracking.
- Use an authorization log that records:
- Date requested
- Portal used
- Clinical documents submitted
- Approval number
- Service dates approved
- Never schedule high-cost services without confirmed approval, unless medically urgent and policy supports retro authorization.
- Audit denied claims monthly to identify authorization trends.
High Audit Risk
Medicaid programs conduct regular audits. These may involve:
- Documentation reviews
- Utilization comparisons
- Overpayment investigations
- Fraud and abuse inquiries
Common triggers include high-level E and M coding, excessive modifier use, or billing patterns outside peer norms.
Recoupments can reach back several years.
The Solution
- Implement internal audits quarterly.
- Randomly sample charts per provider. Compare documentation against billed codes. Identify patterns early.
- Educate providers on medical necessity documentation. For example, a level 4 visit must reflect complexity in history, exam, and decision-making. It cannot rely solely on templated language.
- Maintain organized documentation. During audits, fast and complete responses reduce the risk of escalation.
Claim Denials and Slow Payments
Medicaid denial rates can be higher than commercial plans, especially in managed care.
Common reasons include:
- Incorrect member ID
- Wrong MCO submission
- Missing modifiers
- Authorization mismatches
- Timely filing issues
Each denial adds labor cost and delays revenue.
The Solution
- Track denial reasons by payer monthly. Create a denial dashboard. Identify the top three recurring causes and fix the root issue.
- For example, if 20 percent of denials relate to modifier errors, provide targeted coding education instead of reworking claims repeatedly.
- Submit clean claims within 48 hours of service whenever possible. Faster submissions reduce the risk of late filing.
Medicaid Audits and Compliance Considerations
Medicaid programs conduct routine audits to ensure compliance with billing, coding, and documentation requirements. These audits are designed to identify overpayments, improper billing patterns, and services that do not meet medical necessity criteria.
Audits may include:
- Medical necessity reviews
- Coding accuracy validation
- Documentation completeness checks
- Billing pattern analysis across providers
Common Audit Triggers
- High-level E/M coding without supporting documentation
- Frequent or incorrect modifier usage
- Unusual billing patterns compared to peer benchmarks
- Repeated billing of high-risk or frequently denied services
Even small documentation gaps can lead to recoupments, penalties, or extended audits.
How to Reduce Audit Risk In Medicaid Billing?
Practices can reduce audit exposure by:
- Performing internal chart audits regularly
- Ensuring documentation supports every billed service
- Training providers on medical necessity requirements
- Maintaining organized and accessible records
A proactive compliance approach protects revenue and ensures long-term stability in Medicaid billing.
Struggling with Medicaid Billing Complexity?
Medicaid billing requires constant attention to eligibility changes, payer-specific rules, documentation standards, and managed care variations.
At Medhasty Medical Billing Services, we help healthcare providers:
- Reduce Medicaid claim denials
- Improve clean claim submission rates
- Manage eligibility verification and prior authorizations
- Optimize revenue cycle performance
We support practices across multiple specialties and state Medicaid programs, ensuring compliance with evolving billing requirements. Our team stays aligned with Centers for Medicare & Medicaid Services (CMS) guidelines and state-specific Medicaid requirements to ensure compliance and accurate reimbursement.
👉 Explore our medical billing services
👉 Improve collections with revenue cycle management solutions
👉 Reduce denials with denial management services
Get a Free Billing Assessment Today
Frequently Asked Questions About Medicaid Billing
How long does Medicaid take to pay claims?
Medicaid claim processing times vary by state and payer type. Fee-for-service claims may take 2–4 weeks, while managed care claims can be processed faster depending on the MCO.
What is the timely filing limit for Medicaid claims?
Timely filing limits vary by state and managed care organization. Most Medicaid programs allow 90 to 180 days from the date of service, but missing this deadline can result in claim denial.
Why are Medicaid claims denied?
Common reasons include eligibility issues, missing prior authorization, coding errors, incorrect payer submission, and incomplete documentation.
Does Medicaid require prior authorization for all services?
No, but many services, such as imaging, therapies, and durable medical equipment, require prior authorization depending on the state and MCO.
How can practices reduce Medicaid billing errors?
Practices can reduce errors by verifying eligibility for every visit, ensuring accurate coding, maintaining proper documentation, and implementing structured billing workflows.
What is a clean claim in Medicaid billing?
A clean claim is a claim submitted without errors, complete with all required documentation, coding, and authorization details. Clean claims are processed faster and reduce the risk of denial.
What is Medicaid coordination of benefits (COB)?
Coordination of benefits determines which payer is primary when a patient has multiple insurance coverages. Medicaid is usually the payer of last resort.
Final Thoughts
Medicaid billing is complex because it blends federal oversight with state-level administration and managed care layers. It requires attention to detail, consistent documentation, and proactive denial management.
When handled correctly, Medicaid can be a stable revenue source and expand access to care in your community.
When handled carelessly, it becomes a denial factory.
If you’d like, I can next create a state-specific Medicaid billing guide template that you can customize for your market.



